At the Educating Nurses: A Radical Transformation 2026 Conference last January, Dr. Garrett Chan opened with a provocative question:
What do hoofbeats and a razor have to do with clinical reasoning and implicit bias in decision-making?
The answer is crucial to strengthen nursing education.
Occam’s Razor tells us that the simplest explanation is often the correct one. When we “hear hoofbeats,” we tend to think of horses, not zebras. In many situations, this heuristic helps nurses and clinicians make decisions based on the most likely explanation.
However, in nursing practice, where patients are complex, time is limited, and our human bias can influence our perception, oversimplification can have serious consequences, leading to incorrect clinical judgment.
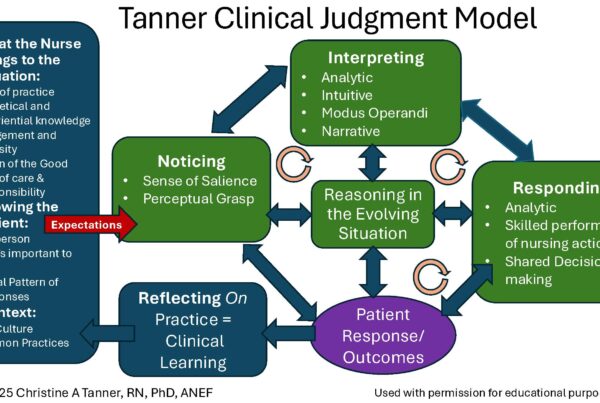
Perceptual Grasp & Salience
Dr. Chan emphasized the importance of perceptual grasp, the ability of the nurse to recognize the particulars of a situation, and a sense of salience (noticing what is most and least important) when using clinical reasoning to make a judgment.
Experienced nurses do not analyze every detail step-by-step. With repeated exposure through direct care, simulation, narratives, and unfolding case studies, they learn to recognize patterns in which salient cues stand out.
For example:
- A subtle change in respiratory effort
- An increase in heart rate
- A patient who “just doesn’t look right.”
Heuristics: Helpful Shortcuts or Hidden Traps?
Heuristics are mental shortcuts that allow clinicians to make quick decisions. For example, if a patient has shortness of breath, one might first assume it is related to a pulmonary issue, but it could also be due to another factor, such as decreased hemoglobin.
If there is ST elevation on an ECG, myocardial infarction (MI) may be suspected. But it could also be something else, such as pericarditis if it is across all 12 leads.
To make accurate judgments, students must learn to reflect and ask questions such as:
- What else could this be?
- What data am I missing and need to collect?
- Does this explanation account for all findings?
Avoiding Clinical Reasoning Biases
Dr. Chan identified the most common biases nurses exhibit in clinical reasoning that need to be recognized and then avoided to make accurate judgments.
These are not character flaws; rather, they are human tendencies that become more pronounced with increased stress, multitasking, and time constraints.
To enhance clinical decision-making, we need to increase students’ awareness of common biases and the typical pitfalls found in clinical reasoning.
- Anchoring Bias
This occurs when individuals fixate on the first piece of information they receive, weigh it too heavily, and fail to adjust to new data that is inconsistent with their assumption.
For example, a newly confused patient may be labeled as “ETOH” withdrawal, and a stroke might be overlooked.
If students are trained to quickly jump to conclusions without assessing new data, they may anchor too early in the reasoning process.
- Diagnostic Momentum
Once a medical diagnosis is made by the provider, it can gain momentum and be accepted, even as new symptoms present that may contradict the initial diagnosis.
For example, a trauma patient is in the ICU complaining of leg pain. The leg x-rays in the Emergency Department were negative for fractures and showed significant soft-tissue swelling. Shift report after shift report emphasizes the leg pain with a negative x-ray for fracture that reinforces the diagnosis of contusions/soft tissue swelling.
However, a nurse questions whether they may have missed something and requests a repeat leg x-ray, which now shows a fracture that was splinted due to soft tissue swelling. Here, the initial negative diagnostic X-ray led clinicians to believe there was no fracture. This is a misdiagnosis and a delay in treatment.
We need to teach students to critically listen to reports, review the medical record, and ask: “What objective data supports this diagnosis?” What has yet to be explored or re-examined?” Or, “Could it be something else?”
- Ascertainment Bias
The stereotypes we hold can shape expectations about patients. So many labels and stereotypes influence our decision-making.
For example, using derogatory terms such as “frequent flier” or “the patient who always uses the call light” influences how we perceive the situation, which, in turn, affects our clinical reasoning and judgment. The danger of making any assumption is that once we do, we have made a judgment and are unable to truly care for this patient.
Discussing assumptions in post-conference or during clinical ensures our graduates provide equitable care.
- Confirmation Bias
Confirmation bias involves seeking information that only confirms your initial impression or pre-existing beliefs. As a result, the nurse may overlook contradictory cues because they have already formed a conclusion.
For example, a patient with a history of opioid use disorder is seen for low back pain, the clinician focuses on the patient’s apparent lack of discomfort and minimizes the patient’s complaint of bowel dysfunction and lower extremity weakness due to cauda equina syndrome.
To increase awareness of this bias, in simulations and classroom discussions, encourage students to consider: “What additional data would challenge your initial judgment?”
- The Unpacking Principle
This bias arises when insufficient information is collected, and the nurse fails to dig deeper and collect additional data when something unexpected presents.
For example, a slight limp after electroconvulsive therapy (ECT) could be regarded as an “expected” finding based on an assumption that is not correct until it turns out to be the result of a stroke that could have been identified if additional assessment data were collected.
- Fundamental Attribution Error
Personal rapport can skew judgment: a nurse may prioritize clinical findings for a well-liked patient while dismissing the same cues from one they find difficult.
For example, if a post-op patient has an unexpected level of pain, the nurse may be more concerned and obtain more data to clarify a concern with a patient who is liked, and disregard the same concern if the patient was labeled a “drug seeker.”
- Overconfidence Bias
This happens when individuals overestimate their own competence and abilities. It is essential to demonstrate humility and recognize your limitations as a student learner.
RaDonda Vaught’s medication error, which involved a medication override she had done numerous times, led to a fatal error of administering vecuronium, a paralytic, instead of Versed, for sedation.
Students should develop habits of double-checking, pausing for reflection, and recognizing their limitations in the face of uncertainty.
- Psych-Out Error
This bias involves assuming that presenting symptoms are solely psychological when they could be caused by a medical problem. Consider all possibilities.
For example, palpitations and anxiety symptoms could mask an underlying thyroid dysfunction.

Clinical reasoning errors or biases are a part of being human. However, teaching students how to recognize and mitigate these errors will strengthen clinical decision-making.
Situated Coaching Questions
As a nurse educator, you are not only a “teacher,” but more of a “coach” who brings out the best in your students by asking the right questions and then carefully listening to their responses to follow up.
Use salient unfolding case studies or the clinical setting to coach your students by asking them questions to assess their perceptual grasp and sense of salience, and to uncover any biases in clinical reasoning.
Here are several reflection questions you can use to strengthen clinical judgment in your students:
- What do you notice that is most/least important?
- What else could cause this?
- Did I consider causes besides the obvious ones? Let me consider an additional 5 causes just to make sure I am reaching the correct diagnosis or conclusion.
- Do I like this patient too little or too much?
- Am I making assumptions about my patient?
- Did I consider alternative perspectives?
- Did I look for both confirming and disconfirming information?

Which questions to unpack clinical bias could you incorporate during clinical or in post-conference debriefing?
Which biases of clinical reasoning have you encountered or experienced most often in your practice?
Share your stories that include your own errors of clinical reasoning so your students can not only learn from you, but also connect with you as a human being who has also made mistakes.
Closing Thoughts
Nursing care is complex; patients are nuanced; bias is real because we are human.
To improve readiness for practice, prioritize teaching your students to recognize the most common clinical reasoning biases, thereby enhancing clinical judgment and the quality of patient care.
References
Chan, G. (2026). Hoofbeats and a Razor; What Do These Have to Do with Clinical Reasoning and Implicit Bias? Educating Nurses 2026, Las Vegas.
Keith Rischer – Ph.D., RN, CCRN, CEN
As a nurse with over 35 years of experience who remained in practice as an educator, I’ve witnessed the gap between how nursing is taught and how it is practiced, and I decided to do something about it! Read more…
The Ultimate Solution to Develop Clinical Judgment Skills
KeithRN’s Think Like a Nurse Membership
Access exclusive active learning resources for faculty and students, including KeithRN Case Studies, making it your go-to resource.